
By: Gideon Lasco, University of Amsterdam
Philippine President Rodrigo Duterte’s bloody war on drugs is just the latest in a region where drug use has usually been met with draconian measures. Thailand embarked 13 years ago on a drug war that strikes eerie parallels with the Philippine situation.
Today, lawmakers in the Philippines are plotting the restoration of the death penalty to bolster the anti-drug campaign. But this, too, is par for the course in the region.
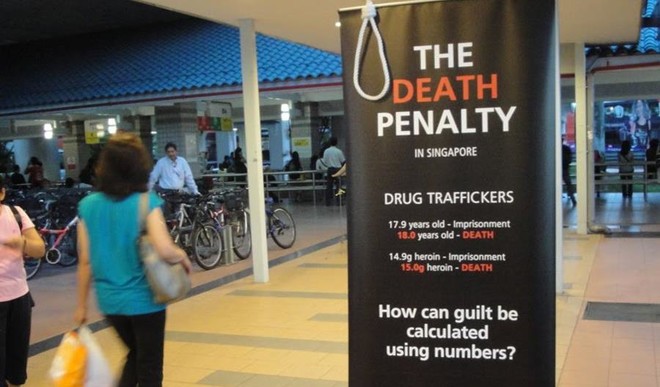
In July 2016, Indonesia executed four convicted drug offenders. On November 17, Singapore executed two men – one Nigerian and one Malaysian – for similar offences.
Reflecting the position of its member states, ASEAN has also adopted a hardline stance, reaffirming the region’s “zero-tolerance approach” to drugs in its annual summit in September.
But there’s broad consensus among researchers that the war on drugs, which typically consists of punitive measures and forced rehabilitation, doesn’t work. And that it’s marked by human rights violations as well as huge social, moral and medical costs.
In one of the most forceful arguments against the drug war, Columbia University neuroscientist Carl Hart stresses that harsh punishments do nothing but prevent young drug users from integrating back into society. And such measures ultimately end up being more harmful than the drugs themselves.

Damir Sagolj/Reuters
What’s worse is that the drug war disproportionately affects the poor and other socially excluded groups, including ethnic minorities. But if the war on drugs doesn’t work, what does?
Successes with harm reduction
At the country level, Portugal’s success story is illustrative. In 2001, the European nation, while not changing the legal status of drugs, changed the way it dealt with drug users.
Instead of putting people in jail, a new law called for their referral to three-person local committees. These committees were given the freedom to consider a range of interventions depending on the user in question.
Those who demonstrate drug dependence are encouraged to seek treatment. Others are discouraged from using drugs through fines and penalties, such as driver’s licence suspensions.
Ten years on, drug use rates have not increased, while drug-related deaths, as well as problematic and adolescent drug use, have decreased.
Portugal’s success, although mirrored by countries such as the the Netherlands, is far from the norm. But even in countries that continue to implement tough approaches, localised interventions are producing promising results. These include nations in Southeast Asia.
In Malaysia, for instance, the implementation of a needle-exchange program has led to a sharp drop in HIV infections among injecting drug users – from a peak of 5,176 in 2002 to 680 in 2014.
In Vietnam, a 2009 methadone maintenance therapy (MMT) program involving 965 opiate users at two sites led to 85.4% and 77.1% reductions in heroin use two years later. This successful pilot led to a scaling-up of the project. By 2014, Vietnam was offering its MMT program in 162 clinics to 32,000 patients.
What these programs have in common is a harm-reduction framework – the idea that the government’s role is to reduce the negative effects of drugs rather than try to eliminate their use entirely. Critics allege that harm reduction actually encourages drug use, but the Portuguese experience, among many others, belies this claim.
A different paradigm
Inez Feria, director of NoBox Philippines, an NGO committed to drug policy reform, has stressed that drug users “have different lives with different stories, and it’s tremendously important to understand, without judgement, each one’s”.
Underpinning successful efforts to deal with drugs, then, must be a paradigm that is open to multiple approaches. This is especially applicable to amphetamine-type stimulants (ATS) such as methamphetamine. As a policy brief drawing from the Thai and Burmese experience states:
Since the pattern of ATS use extends from occasional and recreational use to heavy and dependent use, and only a minority of ATS users fall into the problematic category, the response should vary in accordance with the nature and severity of a person’s involvement with ATS. Different interventions are required to address the complexity of ATS use.
In my research among young methamphetamine users in the Philippines, I met youths who stopped using the drug when they managed to get jobs. Sadly, many were unable to do so, lacking education or the social connections through which to seek assistance.

Staff/Reuters
What’s more, the very stigma associated with drug-use prevents them from being offered opportunities. These findings point strongly to the need to look at “risk environments” – that is, the social and economic contexts in which drug use occurs. They also make the case for considering community-based interventions.
Finding common ground
Harm-reduction approaches can only work if governments and policymakers alike recognise the complexity of the “drug problem”. No single solution exists for all kinds of drug users, or all kinds of drug use.
In what we can see as a silver lining, politicians are beginning to pay more attention to drug issues in their countries. Even in the Philippines, government officials are opening up to alternative approaches. Philippine Secretary of Health Paulyn Ubial, for instance, recently spoke of drugs as a “public health emergency” and a “mental health problem”, in a welcome departure from her president’s rhetoric.
Drug policy advocates can use this common ground as a starting point for engaging with governments. While the evidence is overwhelming that a zero tolerance approach to drugs doesn’t work, it’s also important to steer the conversation towards what does, and nudge leaders in that direction – even if the road is paved with incremental, localised changes.
The example from Vietnam – of a pilot study leading to a scaled-up response – is a promising sign of how research and evidence can change public perception and policies.
The stakes can’t be higher: suspected drug users are being extra-judicially killed and legally executed in the region, even as drug use continues to rise.
What little success harm-reduction advocates can achieve could form the wedge that may finally crack the iron-fisted approach toward drug users. And it may ultimately solve Southeast Asia’s long-standing drug problem.
—
Gideon Lasco, PhD candidate in Medical Anthropology, Amsterdam Institute for Social Science Research (AISSR), University of Amsterdam
This article was originally published on The Conversation. Read the original article.